© 2024 Ferring. Ferring and the Ferring Pharmaceuticals logo and, unless otherwise specified, all product names and service names are trademarks owned by, or licensed to, the Ferring group of companies. All other trademarks are the property of their respective owner(s).
The likelihood of recurrence increases with each subsequent episode
Up to 35%
of patients experience recurrence3,a
Up to 60%
of patients experience subsequent recurrences4
aWithin 8 weeks after initial C. diff diagnosis and successful treatment.
Why is this the case?
A diverse gut microbiome acts as a protective barrier against C. difficile infection (C. diff)5,6
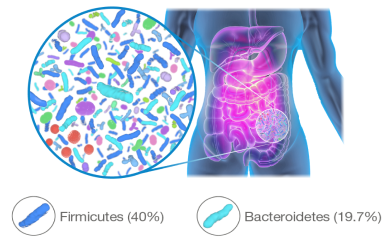
The microbiome is a distinct and essential organ that contains an estimated 100 trillion organisms and is essential to overall health. It influences metabolism and immunity and acts as a barrier for colonization against some pathogenic infections such as C. diff.5-8
Bacteroidetes and Firmicutes are among the most prevalent phyla in the gut microbiome and are vital to inhibiting C. diff and maintaining overall health.6-11
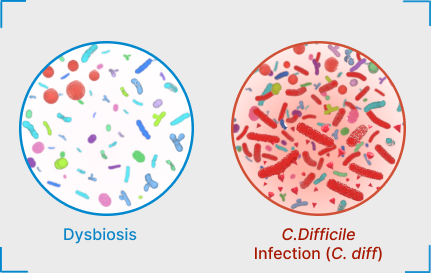
C. difficile infection (C. diff) may proliferate as a result of dysbiosis21-23
Disruption of the composition and diversity of the microbiome (dysbiosis) creates an environment susceptible to pathogenic infection from opportunistic bacteria, such as C. diff. This can lead to a wide spectrum of symptoms ranging from diarrhea to sepsis to mortality.21-23
Dysbiosis may be attributed to multiple factors including medications (i.e., antibiotic use), genetics and lifestyle (i.e., stress, diet, hygiene).24 Dysbiosis is associated with a range of gastrointestinal (GI) and non-GI diseases including neurologic, metabolic, hepatic, inflammatory, and infectious.21,25,26
Antibiotic treatments for C. difficile infection (C. diff) address the acute infection but may worsen dysbiosis, leaving the patient vulnerable to a recurrence. Thus starts a vicious cycle.1,2,27,28
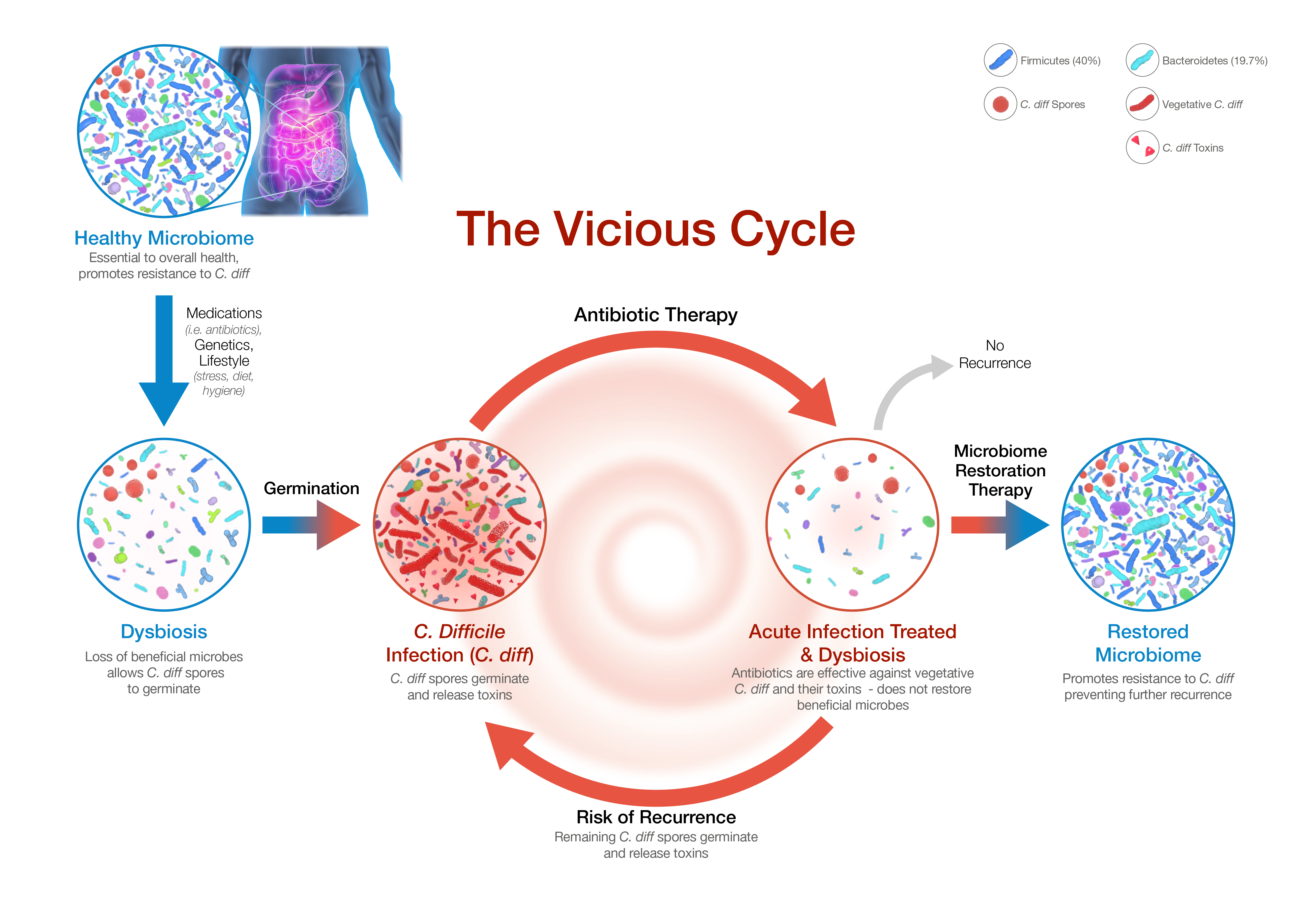
Antibiotic treatment—including vancomycin and fidaxomicin—address the acute infection but do not restore the diverse composition of the gut microbiome and may worsen the state of dysbiosis. This creates a window of vulnerability for recurrence.2,27,28
Secondary bile acids, which are abundant in a diverse microbial environment and may suppress C. diff colonization, are decreased after antibiotics.1,29,30,31
Longer exposure to antibiotics and treatment with multiple antibiotics may increase the risk.32,33
Restoring the gut microbiome may be a promising option for preventing recurrent C. difficile infection (C. diff).34
References
-
Langdon A, Crook N, Dantas G. The effects of antibiotics on the microbiome throughout development and alternative approaches for therapeutic modulation. Genome Med. 2016;8(1):39.
-
DePestel DD, Aronoff DM. Epidemiology of Clostridium difficile infection. J Pharm Pract. 2013;26(5):464-475.
-
Pépin J, Routhier S, Gagnon S, et al. Management and Outcomes of a First Recurrence of Clostridium difficile - Associated Disease in Quebec, Canada. Clin Infec Dis. 2006;42(6):758-764.
-
Leong C, Zelenitsky S. Treatment strategies for recurrent Clostridium difficile infection. Can J Hosp Pharm. 2013;66(6):361-368.
-
Kachrimanidou M, Tsintarakis E. Insights into the Role of Human Gut Microbiota in Clostridioides difficile Infection. Microorganisms. 2020;8(2):200.
-
Antharam VC, Li EC, Ishmael A, et al. Intestinal dysbiosis and depletion of butyrogenic bacteria in Clostridium difficile infection and nosocomial diarrhea. J Clin Microbiol. 2013;51(9):2884-2892.
-
Gilbert JA, Blaser MJ, Caporaso JG, et al. Current understanding of the human microbiome. Nat Med. 2018;24(4):392-400.
-
Thursby E, Juge N. Introduction to the human gut microbiota. Biochem J. 2017;474(11):1823-1836.
-
Wexler AG, Goodman AL. An insider’s perspective: Bacteroides as a window into the microbiome. Nat Microbiol. 2017;2(1):17026.
-
Rinninella E, Raoul P, Cintoni M, et al. What is the healthy gut microbiota composition? A changing ecosystem across age, environment, diet, and diseases. Microorganisms. 2019;7(1):14.
-
Nishijima S, Suda W, Oshima K, et al. The gut microbiome of healthy Japanese and its microbial and functional uniqueness. DNA Res. 2016;23(2):125-133.
-
Faith JJ, Guruge JL, Charbonneau M, et al. The long-term stability of the human gut microbiota. Science. 2013;341(6141):1237439.
-
Elahi M, Nakayama-Imaohji H, Hashimoto M, et al. The Human Gut Microbe Bacteroides thetaiotaomicron Suppresses Toxin Release from Clostridium difficile by Inhibiting Autolysis. Antibiotics. 2021;10:187.
-
Sokol H, Pigneur B, Watterlot L, et al. Faecalibacterium prausnitzii is an anti-inflammatory commensal bacterium identified by gut microbiota analysis of Crohn disease patients. Proc Natl Acad Sci U S A. 2008;105(43):16731-16736.
-
Willing BP, Dicksved J, Halfvarson J, et al. A pyrosequencing study in twins shows that gastrointestinal microbial profiles vary with inflammatory bowel disease phenotypes. Gastroenterology. 2010;139(6):1844-1854.e1.
-
Machiels K, Joossens M, Sabino J, et al. A decrease of the butyrate-producing species Roseburia hominis and Faecalibacterium prausnitzii defines dysbiosis in patients with ulcerative colitis. Gut. 2014;63(8):1275-1283.
-
Tremlett H, Fadrosh DW, Faruqi AA, et al. Gut microbiome in early pediatric multiple sclerosis: a case-control study. Eur J Neurol. 2016;23:1308-1321.
-
Hevia A, Milani C, López P, et al. Intestinal dysbiosis associated with Systemic Lupus Erythematosus. MBio. 2014;5(5):e01548-14.
-
Atarashi K, Tanoue T, Shima T, et al. Induction of Colonic Regulatory T Cells by Indigenous Clostridium Species. Science 2011;331:337–4.
-
Stilling RM, van de Wouw M, Clarke G, et al. The neuropharmacology of butyrate: The bread and butter of the microbiota-gut-brain axis? Neurochem Int. 2016;99:110-132.
-
Bien J, Palagani V, Bozko P. The intestinal microbiota dysbiosis and Clostridium difficile infection: is there a relationship with inflammatory bowel disease? Therap Adv Gastroenterol. 2013;6(1):53-68.
-
Kho ZY, Lal SK. The human gut microbiome—a potential controller of wellness and disease. Front Microbiol. 2018;9:1835.
-
Staley C, Khoruts A, Sadowsky MJ. Contemporary applications of fecal microbiota transplantation to treat intestinal diseases in humans. Arch Med Res. 2017;48(8):766-773.
-
Álvarez J, Real JMF, Guarner F, et al. Gut microbes and health. Gastroenterol Hepatol. 2022;44:519-535.
-
Weiss GA, Hennet T. Mechanisms and consequences of intestinal dysbiosis. Cell Mol Life Sci. 2017;74(16):2959-2977.
-
Riaz Rajoka MS, Shi J, Mehwish HM, et al. Interaction between diet composition and gut microbiota and its impact on gastrointestinal tract health. Food Science and Human Wellness. 2017;6(3):121-130.
-
Knight CL, Surawicz CM. Clostridium difficile infection. Med Clin North Am. 2013;97(4):523-536.
-
Aukes L, Fireman B, Lewis E, et al. A risk score to predict Clostridioides difficile infection. Open Forum Infect Dis. 2021;8(3):ofab052.
-
Ferdyan N, Papazyan R, Walsh D, et al. Rapid restoration of bile acid compositions after treatment with investigational microbiota-based therapeutic RBX2660 for recurrent Clostrioides difficile infection. Open Forum Infect Dis. 2020;7(suppl 1):S15-S16.
-
Theriot CM, Bowman AA, Young VB. Antibiotic-Induced Alterations of the Gut Microbiota Alter Secondary Bile Acid Production and Allow for Clostridium difficile Spore Germination and Outgrowth in the Large Intestine. mSphere. 2016;1(1):e00045-15.
-
Swann JR, Want EJ, Geier FM, et al. Systemic gut microbial modulation of bile acid metabolism in host tissue compartments. Proc Natl Acad Sci U S A. 2011;108(Supp 1):4523-4530.
-
Kelly CP. Can we identify patients at high risk of recurrent Clostridium difficile infection? Clin Microbiol Infect. 2012;18(suppl 6):21-27.
-
Smits WK, Lyras D, Lacy DB, et al. Clostridium difficile infection. Nat Rev Dis Primers. 2016;2:16020.
-
Wilcox MH, McGovern BH, Hecht GA. The efficacy and safety of fecal microbiota transplant for recurrent Clostridium difficile infection: current understanding and gap analysis. Open Forum Infect Dis. 2020;7(5):ofaa114.